


"Varus knee are a relatively common condition in toddlers that may require correction, possibly through surgery, before the end of growth"
WHAT IS IT?
In young children who have recently mastered the ability to walk, careful observation often reveals legs that resemble parentheses. Essentially, it appears as if the knees are separated by a greater space than normal. In almost all children, there is a phase of bow legs, which then tends to progress towards a knock-knee phase. Initially distant, the knees subsequently seem closer together, forming a characteristic X shape. This transition is particularly noticeable around the age of three. Later, the deviated alignment, initially outward and then inward, tends to return to neutral naturally.
IF VARUS KNEE PERSIST
However, varus knee may persist beyond the ages of 3-4 and worsen with growth. This condition results from an imbalance in the activity of growth plates located on the underside of the femur and the upper surface of the tibia, with a tendency for faster growth on the outer side of the knee compared to the inner side.
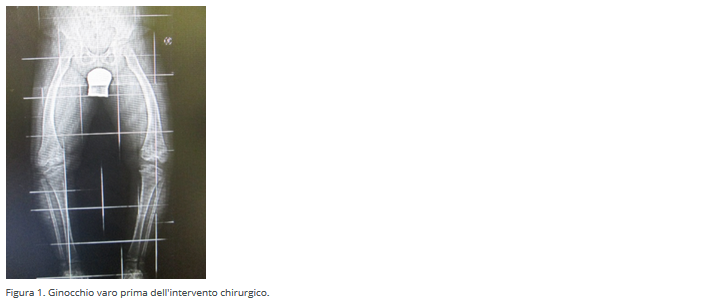
The tibia, the large bone felt when touching the front of the leg, bends inward instead of aligning with the femur. Consequently, the knees move outward, as clearly seen in the X-ray (Figure 1).
SPORTS AND ORTHOTICS CAN HELP
There is no evidence that practicing one sport over another can correct the problem. Insoles and footwear (orthotics) might be helpful, although opinions on their real utility vary, lacking solid scientific evidence.
WHEN SURGICAL INTERVENTION IS NEEDED
If the normal development doesn't improve the knee position, and conservative measures like insoles and footwear prove unsuccessful, surgical intervention may be necessary. The common surgical technique in pediatric cases is epiphysiodesis. This procedure aims to temporarily halt or slow the growth of a growth plate in the femur, tibia, or both, directing growth in the opposite direction of the deformity.
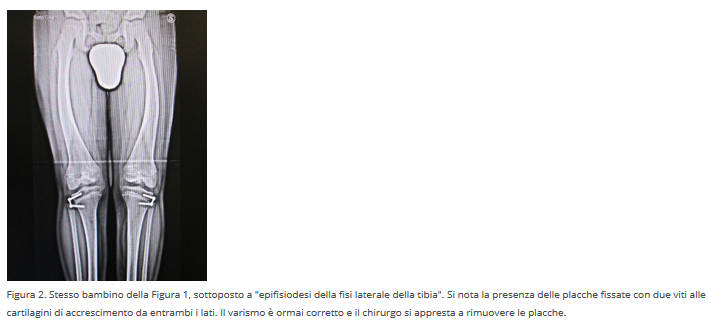
Usually, to correct varus knee, the external growth of the tibial growth plate is temporarily stopped so that the normal growth of the internal part of the same plate leads to realignment. In surgical terms, this procedure is called epiphysiodesis of the lateral tibial physis. The surgery is minimally invasive, involving the application of an eight-plate fixed with two screws across the external part of the growth plate. Recovery times are quick, with the plates remaining fixed to the growth plate until correction is achieved (Figure 2).
This technique is applicable only before the end of growth, typically between the ages of 6 and 13 in girls and 6 and 15 in boys. Once skeletal maturity is reached, more complex and invasive procedures, such as osteotomies, may be necessary, involving the actual removal of bone parts.
SECONDARY VARUS KNEE
Bow legs can be caused by other diseases (secondary bow legs) such as rickets, skeletal dysplasias, and Blount's disease. Blount's disease is characterized by a growth defect in the inner part of the proximal tibia, leading to progressive leg deformities curving below the knee. Blount distinguished two varieties: infantile onset between the first and third year of life and adolescent onset after seven years. Infantile onset is more common, typically affecting obese children who start walking early. The disease's course is marked by increasing bowing of the tibia, usually affecting both sides. Treatment is similar to that mentioned for bow legs.
edited by: Pier Francesco Costici - Orthopedics Operational UnitIn collaboration with: Bambino Gesù - Institute for Health original article from: ufficiobambinogesù.it